Cubital Tunnel Syndrome
If you’ve ever bumped your elbow and felt a tingling sensation down your arm into your hand (hitting your “funny bone”), you’ve bumped the ulnar nerve. But the ulnar nerve also can be the cause of more serious and permanent problems in the fingers and hand.

General Information: Cubital Tunnel Syndrome (Ulnar Nerve at Elbow)
The ulnar nerve extends down the arm, across the elbow, and into the hand. It provides sensation to the little and ring fingers and activates many of the small muscles in the hand. You can actually feel this nerve as it passes behind the elbow and through a tight tunnel (the cubital tunnel) at the inside of the elbow.
The problem an injury to the elbow such as a dislocation or fracture can tear or inflame the ulnar nerve. The inflamed nerve can swell and become trapped in the cubital tunnel. This gives the condition its name, ulnar nerve entrapment. It is often also called cubital tunnel syndrome.
Prolonged pressure on the nerve also can be a problem. Bending the elbow stretches the ulnar nerve and puts pressure on it as it passes through the cubital tunnel, pressing it against the bone. This constant rubbing can damage the nerve’s protective covering (myelin sheath) or the nerve itself and disrupt the nerve’s ability to conduct messages from the brain. Gradually, the muscles of the hand start to weaken, so that it becomes difficult to open a jar or grasp a tool.
Signs of a Problem
 Although the problem is in the elbow area, most symptoms occur in the hand and fingers because the ulnar nerve controls movement and sensation there. Both sensory and motor skills are affected. Symptoms include:
Although the problem is in the elbow area, most symptoms occur in the hand and fingers because the ulnar nerve controls movement and sensation there. Both sensory and motor skills are affected. Symptoms include:
- Tenderness along the inside of the elbow.
- Tingling and numbness in little and ring fingers (especially at night).
- Numbness in your hand when the elbow is bent, such as when you drive or hold a telephone.
- Difficulty with hand coordination (such as when typing or playing a musical instrument).
- Decreased grip and pinch strength; muscle weakness.
- Pain along the inside border of the shoulder blade.
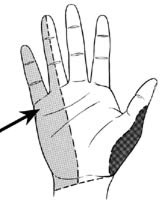
- Tingling and numbness in little and ring fingers (see arrow in diagram) may be a sign of an ulnar nerve problem.
If you experience any of these symptoms, contact a physician. Early diagnosis and treatment is essential to controlling symptoms.
Diagnosing the Problem
A physician can use several methods to diagnose ulnar nerve entrapment. Your own description of the symptoms is a primary source of information. If you’ve experienced a fall, blow or other injury to the elbow, the physician may request an X-ray. The physician may also apply pressure around the nerve to see if pain or tingling results, check to see if the hand muscles are atrophying, or do an electrical stimulation test to see how well the nerve conducts sensory information.
Who’s at Risk
- Anyone who falls on or injures their elbow
- People whose jobs involve excessive bending of the elbow (typists or data entry operators, drivers)
- Diabetics
- People with arthritis or thyroid problems
- Alcoholics
Non-operative (Conservative) Treatment
- Keep the elbow as straight as possible. A straight elbow puts less pressure on the ulnar nerve.
- Avoid crossing your arms across your chest.
- If you frequently use the telephone, consider using a headset or cradle attachment, so you don’t have to hold the telephone to your ear with a bent elbow.
- Adjust your workspace so that you don’t have to bend your elbow more than 30 degrees and you can keep your wrist in a neutral position.
- Consider wearing a splint at night. Something as simple as a towel wrapped around the elbow can help keep it straight.
- Use elbow protectors if you play sports to avoid bumping the elbow.
- If muscle atrophy and numbness continues, corticosteroids may be used to reduce swelling and pressure.
Surgical Treatment
If conservative treatment is not effective and muscle strength continues to weaken, further evaluation and surgery may be needed. There are several surgical options; the most frequent type of surgery (anterior submuscular transposition) moves the nerve from behind the bone to the front of the elbow. After the surgery, treatment must focus on maximizing the use of the hand and arm through physical therapy. This process can take several months.